PGT-SR
PGT-SR is available for most inherited structural chromosome abnormalities that were identified through a karyotype (chromosome study on blood). However, the ability to offer PGT-SR is dependent on the particular chromosome rearrangement in the parent and on the technologies that are available.
What are the steps of the PGT process?
1. Consultation with our team.
2. Complete fertility testing.
3. Case review by the PGT lab.
4. In Vitro Fertilization.
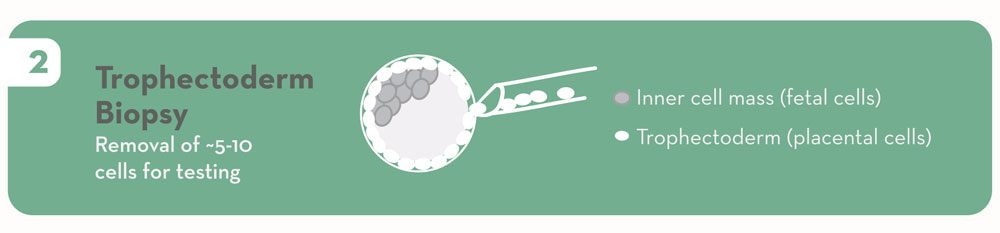
5. Embryo biopsy.
6. Embryos are frozen.

7. Genetic testing for both inherited and sporadic chromosome rearrangements.

8. Results available.
9. Transfer embryo(s) to uterus.
10. Additional embryos are stored for future use.
Is the embryo biopsy safe?
In embryos that have developed to day 5 or 6 (blastocysts), we can see the difference between the inner cell mass (cells that will make the baby) and the trophectoderm (cells that will make the placenta). We are able to safely remove cells from the future placenta without disrupting the baby-making cells. The experience and expertise of the embryologists is very important in minimizing risks to the embryos: <1% of the >10,000 embryos we have biopsied since 2010 did not survive the biopsy. We also believe the long-term risks of blastocyst biopsy to the embryo, pregnancy, and baby to be acceptably low.
Why is the day on which the biopsy is done important?
When genetic testing of embryos first became available, embryos were tested on day 3 at the “cleavage” or 8-cell stage, and only 1 cell was removed for analysis. Now, biopsy techniques and genetic testing methods have evolved to allow for testing on day 5 or 6 of embryo development. ORM only offers testing at this later stage because it is associated with better implantation rates; the ability to biopsy placental (not fetal) cells; and better reliability of genetic results.
How are embryos genetically tested in PGT-SR?
Most times, next-generation sequencing technology can be used to count chromosome fragments and detect large chromosomal imbalances in embryos. Additional genetic test methods may be necessary for cases at risk for smaller chromosome fragments that are difficult to diagnose with the usual technologies.
How do you “make a probe?”
“Probe” is a somewhat outdated term referencing an older technology that required the development of an actual, physical DNA probe that was then used to test embryos. Today, the pre-test process is more a matter of the PGT laboratory reviewing the particular chromosome change for which the embryos are at risk, in order to be sure that an accurate test will be available. The ability to offer accurate PGT-SR is influenced by the specific chromosomal rearrangement in the patient and the technologies that are available to identify “unbalanced” embryos. In most cases, this can be determined within just a few weeks of our clinic submitting the patient’s karyotype (chromosome report) to them, and then the IVF cycle can be planned. This ensures– before an IVF cycle is begun – that an accurate test will be possible. The good news is that in the vast majority of cases, a test can be successfully created and the IVF cycle can move forward.
What is the accuracy of PGT?
Generally the accuracy of PGT is >97%, but the specific accuracy may vary depending upon the particular chromosome abnormality being tested. More detailed information about your particular PGT test becomes available from the PGT laboratory following the lab case review.
Do you recommend screening for sporadic chromosome abnormalities with PGT-A (preimplantation genetic testing for aneuploidy), along with PGT-SR?
Yes. Due to the high rate of sporadic chromosome abnormalities in embryos (30-80%, depending on maternal age), even from healthy, young, or fertile individuals, PGT-A can provide valuable information and help us find the embryos that are most likely to result in a successful pregnancy. Therefore, ORM always performs PGT-A in conjunction with PGT-SR cycles. Both tests can be done simultaneously on the same biopsy, usually using the same technology, and adding PGT-A does not change the overall process or the timeline for results.
Does PGT replace prenatal testing?
Not necessarily. While transferring an embryo that has tested “normal” by PGT is expected to significantly reduce the chance for the future baby/child to have the chromosome abnormality in question, it does not entirely eliminate the risk. Invasive, diagnostic prenatal tests such as chorionic villus sampling (CVS) and amniocentesis are generally considered to be more accurate than PGT (often >99%) and are recommended for those who wish to confirm PGT results in the ongoing pregnancy. Whether or not to have prenatal testing is a personal decision that we recommend discussing in depth with your prenatal provider and a prenatal genetic counselor.
How do I get started with PGT-SR?
We recommend making an appointment for a new patient consultation with one of our physicians to start. You are also more than welcome to email one of our genetic counselors with any initial questions about your specific situation prior to making an appointment.